What is schema theory?
I want to start this post with a fictitious case study.
Imagine that Maeve is a newly graduated nurse a few shifts into her first job in a pediatric emergency department. A 4-year-old arrives with noisy breathing, fever, and visible respiratory distress. Maeve starts her assessment and quickly thinks, “This sounds like croup.” She begins setting up the first-line interventions for the patient: nebulized dexamethasone and cool mist.
Maeve's mentor, a nurse with 10 years of experience, checks in on the patient and notices a few things Maeve missed. The child is in a tripod position (sitting upright and leaning forward), drooling, and can't breathe when they lie down on their back. Their voice sounds muffled, and their fever is 40 °C (104 °F). The mentor recognizes these symptoms don’t fit a typical case of croup, and wonders if the patient might instead have epiglottitis, a more serious condition with a very different treatment plan.
This vignette is a great example of the learning theory called schema theory and shows how it can impact clinical performance.
Schemas are mental frameworks that help us organize disparate pieces of information into a meaningful whole. The theory suggests that instead of remembering dozens of separate details, our brains chunk bits of information into a single idea, concept, or construct that we can more easily recognize and act on. Schemas are how we know how to act in restaurants we've never been in before - either we walk up to the counter and order or wait to be handed a menu and seated. Because we have schemas in mind for how fast-food and slow(er) dining restaurants function, we understand how to behave given our established mental schemas from other restaurants that we've built over time.
Essentially, you can think of a schema like a cluster of interconnected nodes that pull together observations and experiences that we've collected and remembered over time. Each node is a bit of information, such as a symptom, a risk factor, or an action treatment option for a specific condition. Some nodes may only have a single connection to them, whereas others may have many interconnections with other nodes. The more connections a node has, the easier it is to retrieve that bit of information when you need to think about it.
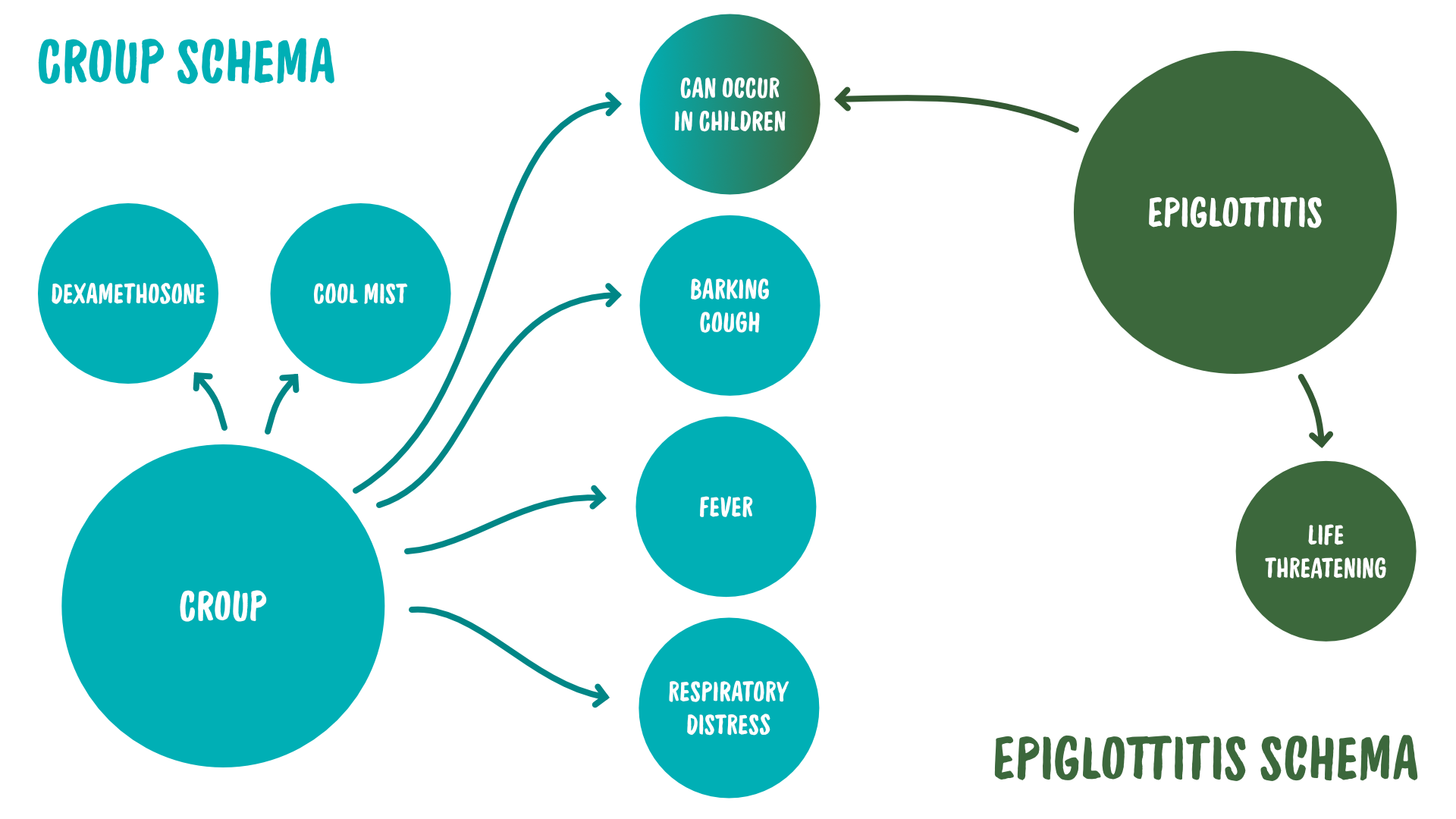
In our story, Maeve has a developing schema for croup - it's quite common, so she's saw it often during her training and has more experiences and observations to draw on - but her schema for epiglottitis is poorly developed. She may remember from lectures in school that epiglottitis is rare and a serious respiratory illness that can present in pediatric patients, but she doesn't really know how it presents and what symptoms it shares with other respiratory conditions.
To illustrate, Maeve’s schemas for croup and epiglottitis might look like this:
Her preceptor, on the other hand, has much more refined schemas for both of these conditions, thanks to her years of experience.
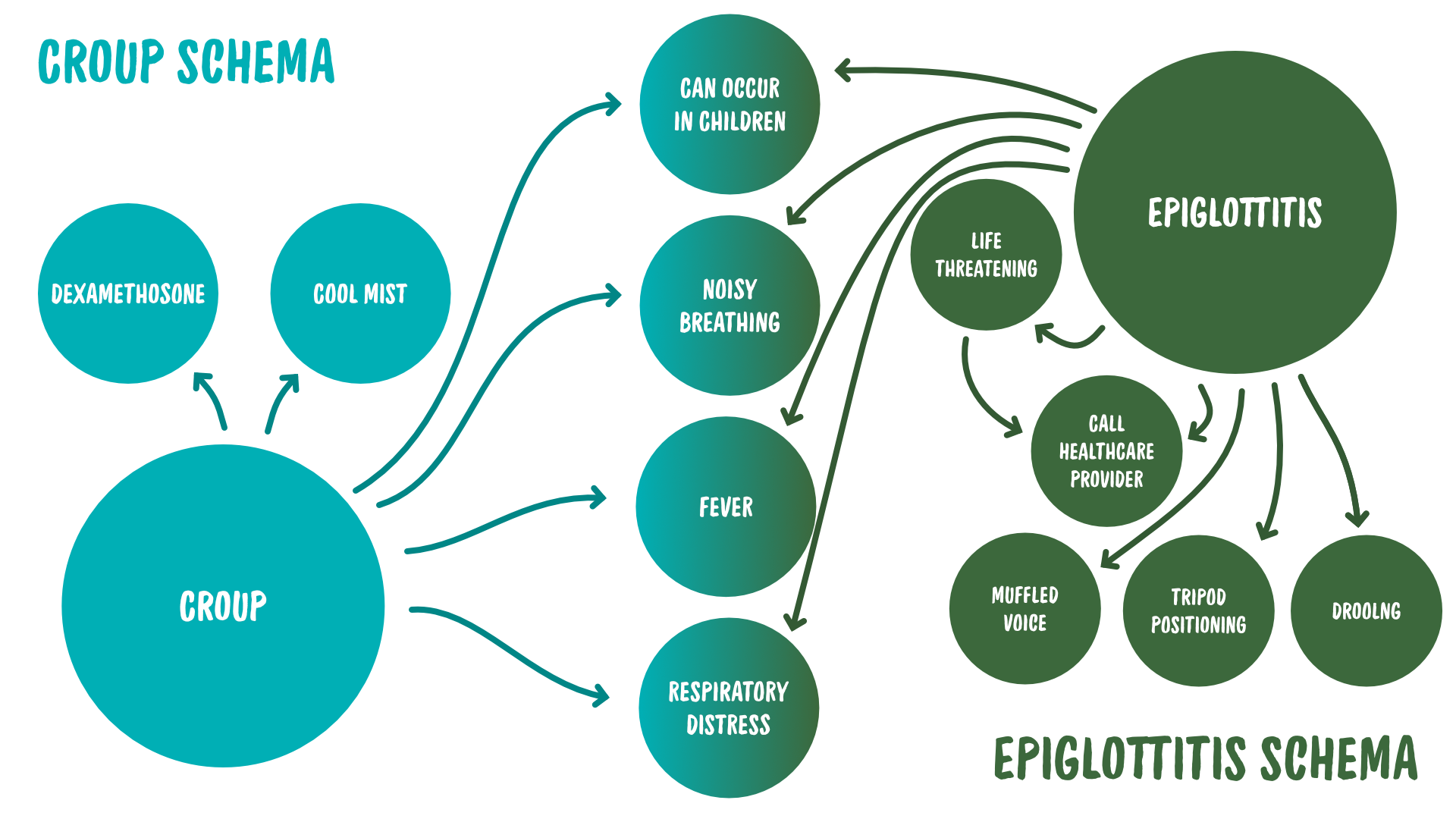
You can see the difference, not just in the node count, but also how interconnected each node is to the others within the schema.
Assimilation and accommodation
Piaget's famous theory of cognitive development integrates well with schema theory. When someone learns something new (or has a novel experience), one of three things can happen:
- Assimilation: The person fits the new information into an existing schema. Assimilation requires less mental work from learners because they are connecting new nodes to existing nodes. In essence they are just modifying their understanding of an existing concept they know by appending the new information - kind of like tacking it on at the end of a list. So, to use our earlier example, Maeve could incorrectly assimilate epiglottitis as a form of “severe croup,” one that has the same treatment plan as croup. (Please note that this would be incorrect given the example!)
- Accommodation: The person builds a new schema (or substantially reshapes an old one). Accommodation requires more mental effort than assimilation does because it's much harder to create a new mental model of something that isn't well anchored in existing schemas. In essence, we have to build a whole new mental model based solely on this single piece of new information, or this one observation or experience, with only a few tentative nodes from other, related schemas to help ground the new schema. To use our earlier example again, Maeve could learn that epiglottitis is a distinctly separate condition, but some of its symptoms overlap with other upper respiratory conditions, including croup.
- No change: The person rejects the new information and doesn’t update their existing schema at all. In the case of our example, this would result in Maeve incorrectly refusing to believe that epiglotitis exists at all.
So that's what schemas are, how we form them, and how they might or might not change given new information or experiences.
Building better schemas
Knowing all of this, are there strategies that can help us build better schemas and build them more quickly? Yes. Overall, from the schema theory lens, when teaching something new to learners, our goals should be to:
- Activate what learners already know related to the new information
- Make relationships between similar ideas explicit (instead of hoping learners infer them), and
- Get learners to retrieve and use these schemas repeatedly over time.
Here are some ways we can achieve these objectives in practice. I'll continue using the example of croup to help illustrate these points:
- Do frequent, quick retrieval. Initiate a teachable moment and give yourself 5 to 10 minutes of review with the learner. You could ask the learner questions like, “What are your red flags for respiratory distress in kids?” and have them connect these to as many illnesses as they can remember. Then, you could watch a couple of short videos on YouTube of patients with respiratory distress and ask learners to name the key symptoms they see.
- Group similar conditions together.
When teaching upper respiratory diseases to learners for the first time, teach croup alongside what it’s confused with in real life: bronchiolitis, asthma, foreign body aspiration, epiglottitis, pneumonia, and so on. Then, ask your learner to compare and contrast the conditions, like “What would signal to you that your patient has croup and isn't instead in the middle of an asthma attack?” Fun fact: This is why most of the textbooks on diagnosis are organized by symptoms, and not by organ system. They are trying to build strong schemas! - Use case variation. When running case-based scenarios with learners, present sets of cases that differ on one key clinical feature, and have learners reflect on how that single difference changes the patient's care plan. For example, one at a time, vary the patient's age, onset (gradual vs. sudden), severity of fever, overall hydration and appetite, and the severity of the patient's work of breathing, and ask how the diagnosis and treatment would shift based on each single-variable change.
- Avoid ambiguity. When discussing teaching or reviewing clinical conditions, use descriptors that the learner can explicitly observe. It's most important to avoid using vague descriptions, like “the patient looks toxic,” or “they look bad,” or “they're working hard.” Instead, be specific and direct with your observations: the patient might be exhibiting retractions, nasal flaring, head bobbing, grunting, stridor at rest, cyanosis, or decreased responsiveness. We want to tie these concrete observable symptoms to the learner's newly forming schema. Vague terms make learners have to work unnecessarily harder to link these symptoms together in their schema, and they're more likely to make errors as a result.
- Highlight your decision making pathways. When working with patients, say your clinical reasoning out loud. This will help the learner connect the treatment to their existing schema directly, rather than making inferences based on what the teacher is doing (which, again, could lead to faulty schemas and errors in the future). For example, “Stridor at rest plus retractions makes me worry about significant upper airway obstruction. I'm concerned, I think we need to call for more support now.”
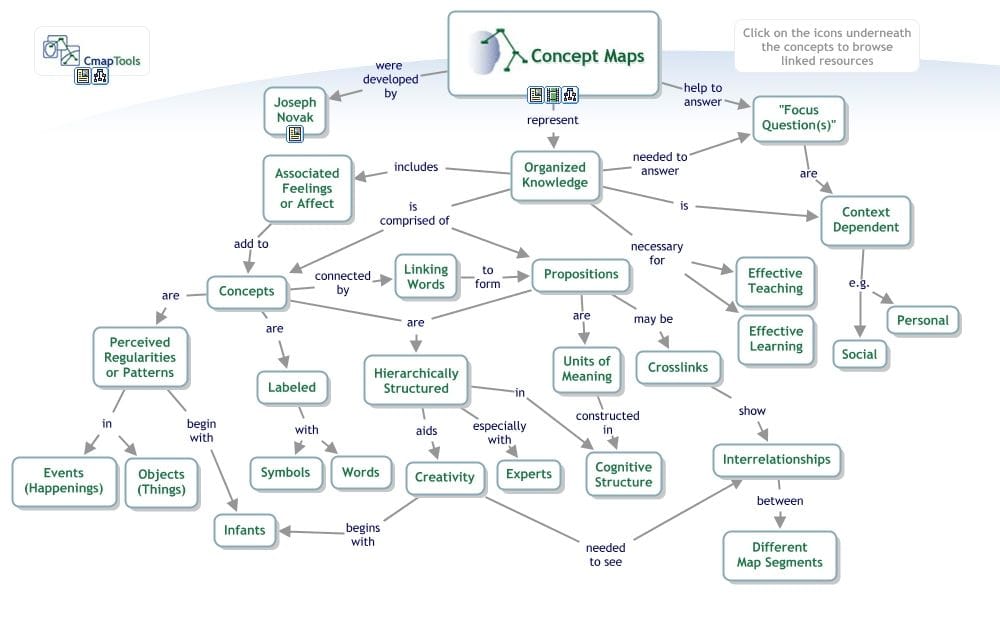
- Have learners build concept maps or flowcharts. Encourage learners to create a visual map of their schemas by building mind maps or flow charts. The act of creating this map will force them to think deeply about how each concept relates to each other and to clarify any misunderstandings in their existing schemas. Have them revisit their mind map every now and again to help them recall these connections, especially if they haven't seen that patient type or clinical presentation for a while.
Key takeaways
So, in summary:
- Schemas are a web of interconnected ideas that help us organize information into meaningful mental frameworks.
- The more interconnected these ideas are, the stronger we remember them and the easier it is to remember them.
- It's good teaching practice to make the relationships between ideas within a schema or between schemas explicit and give learners repeated chances to retrieve and apply the right schema.
References
- Concept map image. Author: Dvitalo12 License: CC-BY-SA
{kind=link}
Member discussion